https://leisureguy.wordpress.com/2020/03/09/the-many-worlds-hypothesis-is-probably-true/
Fictional depictions abound, such as in my books in The Spanners Series!
https://leisureguy.wordpress.com/2020/03/09/the-many-worlds-hypothesis-is-probably-true/
Fictional depictions abound, such as in my books in The Spanners Series!

#COVID19 / #Coronavirus Updates and Info Sources
As some of you know, my mom (almost 88, but mostly healthy) and I (65) live in St. Louis County, Missouri, USA, which just “confirmed” its first case of the #Coronavirus. It exists in a young woman who was allowed to return from ‘studying abroad” Italy last week unencumbered (!?!). She went to a hospital that is and therefore must live very close to us.
Who knows where she went, who else she contacted/infected, who her people are, etc.? No other info was made available, so I am feeling very cautious locally for the first time.
My mom, however, is in huge denial and refuses to cancel her four-times weekly mah jong gatherings/games with 4 – 5 elderly women (she is one of the youngest!) this week (3/8/20).
I, however, after reading up on all this, am beginning to ‘stockpile” toilet paper (not too much), tissues, non-perishable or less-perishable food, and put out the Hydrogen Peroxide spray and paper towels for her to use when she returns each day, to wipe down the handles of her cart and/or walker.
We are also going to cleanse her mah jong tiles each afternoon after she returns.
They eat lunch there twice/week, and use the bathroom frequently; plus, others use the same space (the condo’s “clubhouse”), so who the hell knows what anyone is carrying and/or shedding??). I begged her to demand that her friends to WASH THEIR HANDS every time they leave the table for any reason, before returning to play. She is pooh-poohing that request (so far).
I finally decided: if this is what kills her, so be it. At least she’s having fun. Not kidding. I’m a Buddhist, so we take a common-sense approach to everyone’s inevitable demise.
Not wishing death on anyone any time soon, but since these articles and stats are likely to be correct, we are ALL going to lose friends and loved ones, or our own lives, before this is “finished,” if it ever is…. Buckle up.
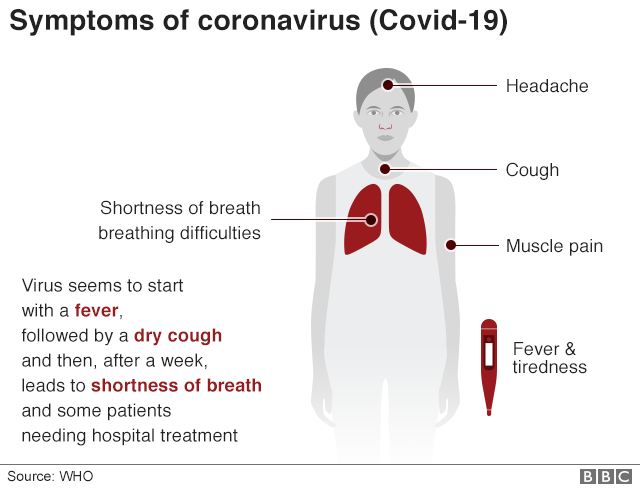
And, if you’re not sure if what you’re sneezing, coughing, or aching about is this virus, check here:
So, FYI: Some great sources, in detail, below, and links, first, for more info.
Please make sure the info you “follow” is reliable, accurate, and trustworthy!
Stay safe and well. In case you are thinking: Oh, don’t be such an alarmist, read this, of the CLOSING DOWN of main population centers in Italy this weekend (3/7/20): https://www.bbc.com/news/world-middle-east-51787238?fbclid=IwAR2yMGdBkvhyn8Kyae9Xt6P_dSqebjXWGbsN31Ut8EZuRTaL5GQ8MFs06qM
When/if you are self-quarantined or hospitalized and want to read utopian, romantic, non-violent sci-fi, buy my 3 ebooks and/or paperback books! Give them as gifts. Why not? http://www.sallyember.com/Spanners
Sally Ember, Ed.D. (NOT A DOCTOR OF MEDICINE)
A) One excellent ongoing and frequently updated source, here, is Germ Info, http://germinfo.org which is excellent. Read and share from there and/or on Facebook: https://www.facebook.com/groups/germinfo/permalink/2311603802276736/
B) A little light in the tunnel, for this horrible time, from Stanford University Labs: a faster and soon-to-available corona virus test kit for USA use: https://www.sacbee.com/news/california/article240974406.html

D) More good info about what to expect regarding the USA and global experiences of the #COVID19 pandemic (and a bit less discouraging in some places; more, in others), from Juliana Grant, MD, MPH:
“Coronavirus: an email to my family”
[not mine; this woman–info, below–who is a public health expert]
“Notes: I originally wrote this to share with my family and close friends. It’s now getting passed around so I’m posting it publicly. I have revised the language slightly a few times. This is the most current version.”
“Hi folks,
“A number of you have asked me what I think is going to happen with coronavirus (COVID-19) and what we should be doing to prepare. I have a few thoughts about what’s likely to happen and what you can do about it. For those of you who don’t know me well, I am a preventive medicine physician and infectious disease epidemiologist. I graduated from the CDC’s Epidemic Intelligence Service and have over 17 years of experience in the field, most of that with CDC.
“Wishing everyone good health,
“Juliana”
—“Who[m] should you listen to?”
“The CDC and your state health department are your best place for information about COVID-19. (Listen to them before you listen to me.) Be cautious about other sources of information – many of them will not be reliable or accurate.
—“How bad is this going to be?”
“It’s possible that COVID-19 will be similar to a bad flu year but there are a number of indications that it will be very much like the 1918 Flu Pandemic. To put that in perspective, the 1918 flu did not end civilization as we know it but it was the second-deadliest event of the last 200 years. It is likely that people you know will die from COVID-19.
“However, there is one critical difference between COVID-19 and the 1918 flu – the 1918 flu virus hit children and young adults particularly hard. COVID-19 seems to be most severe in older adults. Children and young adults generally have mild infections and we are grateful for this.
—“What can we expect?”
“This is not the zombie apocalypse. Core infrastructure (e.g., power, water, supermarkets, internet, government, etc.) will continue to work, perhaps with some minor disruptions.
“There will be significant economic disruption: a global recession is very possible and there will probably be significant shortages of some products. The healthcare system will be hit the hardest. The number of people who are likely to get sick is higher than our healthcare systems can probably handle.
“Daily life will be impacted in important ways. Travel is likely to be limited and public gatherings will probably be canceled. Schools will probably be closed. Expect health departments to start issuing these orders in the near future, especially on the West Coast.
“The acute pandemic will probably last at least for several months and quite possibly for a year or two.
—“What can we do?”
“We can’t keep COVID-19 from being a global pandemic but the more we can do to slow the spread of the disease, the less severe the impact will be. With that in mind, here are the things you can do:
—–“Stay calm but take it seriously. This will likely be bad but it’s not the apocalypse.
—–“Stay home if you’re sick or someone in your house is sick.
—–“Leave medical supplies for healthcare workers. You shouldn’t be stockpiling masks or other medical supplies. They are needed in hospitals to keep our healthcare workers healthy.
—–“Wash your hands. Get in the habit of frequently washing your hands thoroughly and covering your cough.
—–“Minimize your exposure. Now that we’re seeing community transmission in the U.S., it’s probably time to start cutting back on your exposure to other people. Depending on your circumstances, consider:
——-“Canceling non-essential travel
——-“Avoiding large-scale gatherings
——-“Working from home if possible
——-“Minimizing direct contact with others including hand shakes and hugs
——-“Reducing your trips out of the house. If possible, shop for two weeks of groceries at once or consider having your groceries delivered. Stay home and cook instead of going to a restaurant.
——-“Remember, keep calm and prepare. This is likely to be bad, but if we respond calmly and thoughtfully, we can handle it.
“Feel free to share this [email] as you see fit.”
from: https://www.julianagrant.com/blog/2020/2/29/coronavirus
E) If you’re ready for very sobering stats about the trajectory of this, that we are all facing NOW and soon:
“I am sharing this with you because many people have not yet started preparing. For schools being out. Work being out. No parties. No restaurants. No gatherings. No Uber. No eating out. This may make you panic or worry a lot. This is what I see happening. In 6 weeks from now. Not only in America. In every country.
“That’s why I tell you to cancel all you travel plans. Cancel any parties you are going to or organizing. I want you to protect your family. The only way to get ahead of this is to minimize human to human contact until we have diagnostics, vaccines, medications. I believe all schools should close soon. Very soon. Do not read if you are already panicked!”
“From Liz Specht on Twitter, @LizSpecht
“‘I think most people aren’t aware of the risk of systemic healthcare failure due to COVID19 because they simply haven’t run the numbers yet. Let’s talk math. Let’s conservatively assume that there are 2,000 current cases in the US today, March 6th. This is about 8x the number of confirmed (lab-diagnosed) cases. We know there is substantial under-Dx due to lack of test kits; I’ll address implications later of under-/over-estimate.
‘We can expect that we’ll continue to see a doubling of cases every 6 days (this is a typical doubling time across several epidemiological studies). Here I mean *actual* cases. Confirmed cases may appear to rise faster in the short term due to new test kit rollouts.
‘*** We’re looking at about 1M US cases by the end of April, 2M by ~May 5, 4M by ~May 11, and so on.
‘*** Exponentials are hard to grasp, but this is how they go. As the healthcare system begins to saturate under this case load, it will become increasingly hard to detect, track, and contain new transmission chains. In absence of extreme interventions, this likely won’t slow significantly until hitting >>1% of susceptible population.
‘What does a case load of this size mean for healthcare system? We’ll examine just two factors — hospital beds and masks — among many, many other things that will be impacted.
‘The US has about 2.8 hospital beds per 1000 people. With a population of 330M, this is ~1M beds. At any given time, 65% of those beds are already occupied. That leaves about 330k beds available nationwide (perhaps a bit fewer this time of year with regular flu season, etc). Let’s trust Italy’s numbers and assume that about 10% of cases are serious enough to require hospitalization. (Keep in mind that for many patients, hospitalization lasts for *weeks* — in other words, turnover will be *very* slow as beds fill with COVID19 patients).
‘By this estimate, by about May 8th, all open hospital beds in the US will be filled. (This says nothing, of course, about whether these beds are suitable for isolation of patients with a highly infectious virus.) If we’re wrong by a factor of two regarding the fraction of severe cases, that only changes the timeline of bed saturation by 6 days in either direction. If 20% of cases require hospitalization, we run out of beds by ~May 2nd. If only 5% of cases require it, we can make it until ~May 14th. 2.5% gets us to May 20th.
‘This, of course, assumes that there is no uptick in demand for beds from *other* (non-COVID19) causes, which seems like a dubious assumption. As healthcare system becomes increasingly burdened, Rx shortages, etc, people w/ chronic conditions that are normally well-managed may find themselves slipping into severe states of medical distress requiring intensive care & hospitalization. But let’s ignore that for now.
‘Alright, so that’s beds. Now masks.
‘Feds say we have a national stockpile of 12M N95 masks and 30M surgical masks (which are not ideal, but better than nothing). There are about 18M healthcare workers in the US. Let’s assume only 6M HCW are working on any given day. (This is likely an underestimate as most people work most days of the week, but again, I’m playing conservative at every turn.)
‘As COVID19 cases saturate virtually every state and county, which seems likely to happen any day now, it will soon be irresponsible for all HCWs to not wear a mask. These HCWs would burn through N95 stockpile in 2 days if each HCW only got ONE mask per day.
‘One per day would be neither sanitary nor pragmatic, though this is indeed what we saw in Wuhan, with HCWs collapsing on their shift from dehydration because they were trying to avoid changing their PPE suits as they cannot be reused. How quickly could we ramp up production of new masks? Not very fast at all. The vast majority are manufactured overseas, almost all in China.
‘Even when manufactured here in US, the raw materials are predominantly from overseas… again, predominantly from China. Keep in mind that all countries globally will be going through the exact same crises and shortages simultaneously. We can’t force trade in our favor.
‘Now consider how these 2 factors – bed and mask shortages – compound each other’s severity. Full hospitals + few masks + HCWs running around between beds without proper PPE = very bad mix. HCWs are already getting infected even w/ access to full PPE. In the face of PPE limitations this severe, it’s only a matter of time.
‘HCWs will start dropping from the workforce for weeks at a time, leading to a shortage of HCWs that then further compounds both issues above. We could go on and on about thousands of factors – # of ventilators, or even simple things like saline drip bags.
‘You see where this is going. Importantly, I cannot stress this enough: even if I’m wrong – even VERY wrong – about core assumptions like % of severe cases or current case #, it only changes the timeline by days or weeks.
‘This is how exponential growth in an immunologically naïve population works. Undeserved panic does no one any good. But neither does ill-informed complacency. It’s wrong to assuage the public by saying “only 2% will die.”
‘People aren’t adequately grasping the national and global systemic burden wrought by this swift-moving of a disease. I’m an engineer. This is what my mind does all day: I run back-of-the-envelope calculations to try to estimate order-of-magnitude impacts. I’ve been on high alarm about this disease since ~Jan 19 after reading clinical indicators in the first papers emerging from Wuhan.
‘Nothing in the last 6 weeks has dampened my alarm in the slightest. To the contrary, we’re seeing abject refusal of many countries to adequately respond or prepare.
‘Of course, some of these estimates will be wrong, even substantially wrong. But I have no reason to think they’ll be orders-of-magnitude wrong. Even if your personal risk of death is very, very low, don’t mock decisions like canceling events or closing workplaces as undue “panic”. These measures are the bare minimum we should be doing to try to shift the peak – to slow the rise in cases so that healthcare systems are less overwhelmed.
‘Each day that we can delay an extra case is a big win for the HC system. And yes, you really should prepare to buckle down for a bit. All services and supply chains will be impacted. Why risk the stress of being ill-prepared?
‘Worst case, I’m massively wrong and you now have a huge bag of rice and black beans to burn through over the next few months and enough Robitussin to trip out. One more thought: you’ve probably seen multiple respected epidemiologists have estimated that 20-70% of world will be infected within the next year.
‘If you use 6-day doubling rate I mentioned above, we land at ~2-6 billion infected by sometime in July of this year. Obviously I think the doubling time will start to slow once a sizeable fraction of the population has been infected, simply because of herd immunity and a smaller susceptible population.
‘But take the scenarios above (full beds, no PPE, etc, at just 1% of the US population infected) and stretch them out over just a couple extra months. That timeline roughly fits with consensus end-game numbers from these highly esteemed epidemiologists. Again, we’re talking about discrepancies of mere days or weeks one direction or another, but not disagreements in the overall magnitude of the challenge.
‘This is not some hypothetical, fear-mongering, worst-case scenario. This is reality, as far as anyone can tell with the current available data.
That’s all for now. Standard disclaimers apply: I’m a PhD biologist but *not* an epidemiologist. Thoughts my own. Yadda yadda. Stay safe out there.'”
F) What about a vaccine? Israel claims to be able to have one ready near the end of April, or by mid-May, 2020, but “Anthony Fauci, the longtime director of the National Institute of Allergy and Infectious Diseases (N.I.A.I.D.) [in the USA], spoke up. ‘A vaccine that you make and start testing in a year is not a vaccine that’s deployable,’ he said. The earliest it would be deployable, Fauci added, is ‘in a year to a year and a half, no matter how fast you go.’”
https://www.newyorker.com/news/news-desk/how-long-will-it-take-to-develop-a-coronavirus-vaccine
Trials/testing take more than a year, but this just got released (3/8/20):

Sharing books, author voices, and news from the University of Washington Press
Where Adventure, Lifestyle, and Food Come Together
It's a beautiful day in the neighborhood.
Every Second Thursday | 5-8pm
A novelist with a passion for reading and traveling shares his view of the world and his adventures.
Rejuvenate, relax and revitalize with holistic healing.
Information & Analysis on Global Mass Transit Industry
Stories to warm the furry heart and soul
Local Burien News and Stories that support Human Flourishing and Balanced Community Conversations. Topics include Education, Government, Sports, Lifestyle and Community Perspectives.
Updates from King County's School-based Partnerships Program
Community News For All of Seattle's Capitol Hill
News that connects you
An interdisciplinary research project on cities and the night.
Manhattan's little, quieter island and beyond
Smile Always
#Evola #Traditionalism #Metaphysics #Initiation #Esotericism #JuliusEvola #SpiritualHierarchy #Transcendence

You must be logged in to post a comment.