Advocacy, Entitlement and Knowing When to Complain: The Rights of Poor People
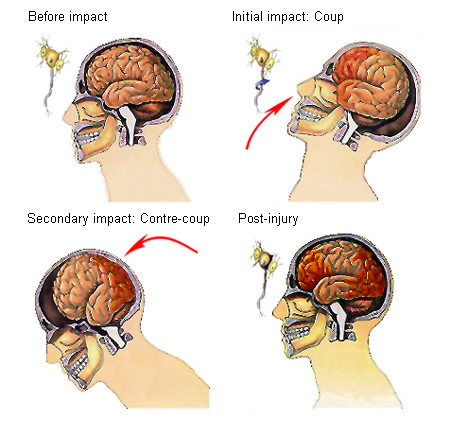
If you are new to this blog, you may not know that I was in an accident about two years ago that resulted in a broken nose and concussion as well as other injuries. The concussion was not one of the “good” kind, meaning, I have still not completely recovered.
This deterioration in my health caused me to run through my savings and unemployment benefits in California and have to rely on others. Finally, I am privileged to benefit from my mother’s having space and a generous heart, allowing me to move in with her in St. Louis about 18 months ago.
Missouri, however, is not a great place to live if you are indigent. This post is the third in a series about my experiences here. This third one is on poor people’s rights. The second was on food for indigent people in Missouri (published February 16, 2016, http://wp.me/p2bP0n-1BL). The first one was on health care (published February 9, 2016, http://wp.me/p2bP0n-1By).
This post is important because it looks at the underlying issues that make a difficult situation (being poor) worse or better for each person. The intersections of perceived or claimed race/ethnicity, perceived or claimed gender, perceived or claimed social class, perceived or claimed age, home/best language, physical and mental health and (dis)abilities, perceived or claimed religion, perceived or claimed sexual orientation, and economic status in the city of St. Louis, Missouri, USA, in the mid-20teens, can adversely influence, improve or neutrally affect one’s experiences every moment.
“Intersectionality” is an important part of understanding how poverty impacts each person and family differently. Therefore, in this series, I need to bring in the politics of social identity. We all have to learn to address these overlapping oppressions and unfair treatments to help ourselves understand how everything is NOT actually “equal” regardless of the similarities in two people’s incomes.

Intersectionality includes all of these components of one’s social identity.
It’s not “all good.”
It doesn’t have to be this way.
It ISN’T what it IS “naturally”: people and then institutions run by people make things this way and create/perpetuate systems that keep them this way.
Missouri is one of the worst places to be if you’re poor, but it’s not even the worst by any standards. Your experience all depends on the other components of your social identity. If you’re believed to be a white male, seemingly in good health and able-bodied, perceived to be heterosexual, assumed to be Christian, speaking mid-Western-accented English like a native, have at least some college education and otherwise seeming to be a USA “mainstream” guy between the ages of 25 – 65, you are going to be much better treated and fare better even when you’re poor than if you do not claim or cannot pull off having others believe you have all or any of those social identities.
If you’re also not a felon, have a place to live (a legal address) and (the use of) a car, you’re probably not going to be poor for very long.
Unless you’re obese. Unless you’re smelly. Unless you’re an addict. Unless you’re perceived to be “not one of us” in whatever way “us” is defined: then, you’re in some trouble. But, even with those cards stacked against you, as a poor assumed-to-be-white & -Christian with some education who speaks adequate English and can pass for straight and male and under age 65, you’re still going to be better off than anyone who isn’t.

Change one aspect—gender—and things automatically get much worse. Change two—ethnicity/race and gender—and you’re doomed.
Check this out, from Everyday Feminism, June 20, 2015 by Carmen Rios “These 5 Statistics Prove That We’re Feminizing Poverty (And Keeping Women Down in the Process)” http://everydayfeminism.com/2015/06/feminizing-poverty/
— “Despite the overall poverty rate declining in America, 18 million women remain below the poverty line.”
—“Women are poorer than men in every state, regardless of education or geographic location. And for women of color, elderly women, and LGBTQIA+ women, it’s even worse.”
—“The poverty rate for Native American, Black, and Latina women is almost double the poverty rate for white women.”
—“For women, and especially women of color, the fight to raise the minimum wage to $10.10 or $15 is very personal—and could be the difference, for them, between barely surviving and finally thriving.”
—“…over a lifetime, women lose an average of $434,000 to the wage gap.”
—“One of the most important aspects of intersectional feminism is the understanding that when we fight for the most marginalized women, we liberate all women along with them.”
And, from other sources (see below) that add in education and other factors to race/ethnicity and gender with income levels:
—“White households take home between $10,000 to $20,000 more per year than their Black counterparts in every age bracket”
—“Enrollment in ‘high poverty’ schools for Black children is 41 percent, 38 percent for Hispanic children, 31 percent for American Indian/Alaska Native and a mere six percent for Whites.”
—“Even when Black and minority children attend mixed schools, they are more likely to be tracked into remedial or basic classes while their White counterparts take advanced, honors level courses.”
—“70 percent of students arrested or referred to law enforcement for school-related infractions were Black or Latino.”
—“While people of color only comprise about 30 percent of the US population, they account for 60 percent of those imprisoned.”
—“There is no such thing as unbiased, unpolitical education.”
—“People with ‘Black’ or ‘ethnic-sounding’ names are less likely to get callbacks for interviews.”
—“Blacks are more likely to be born into poverty and are less likely to escape it.”
—“Whites are 2-3 times more likely to make it into the middle class in their lifetimes compared to their black counterparts.”

from http://iamarevolutionary.wordpress.com
Poverty IS violence. It has to stop.
Find a well-vetted nonprofit that advocates and works to end poverty and understands intersectionality and contribute, volunteer, blog about their work! Here is one: http://www.results.org/
Good news! We made this mess; we can clean it up.

Nelson Mandela, Audre Lorde, Martin Luther King, Jr., Angela Davis, Gloria Steinem and so many more have spoken out about the nature of the human-made elements of our social and political systems and the oppressions they systematize.
WE are the ones who must advocate, complain, recognize that we are entitled to better and that so is everyone else, and ACT!
—Do not sit by and watch passively when others are mistreated, disrespected, unfairly scheduled or managed, especially when you are in any position of better privilege: it is your DUTY to advocate whenever you are able.
—Write letters, blog, make phone calls, picket, march, show up and let those in power know you are not satisfied with the “status quo.” Be specific.
—VOTE! It is your DUTY and responsibility as a USA citizen who can vote (if you are one) to use that right in EVERY election. It is the LOCAL elections that most affect people who live near you, and regional and state office holders who make laws that affect us all. Federal elections matter, too, but not as obviously or as immediately.
 I VOTE! And, as of early March, I am working as a election-day supervisor at a local polling place!
I VOTE! And, as of early March, I am working as a election-day supervisor at a local polling place!
—THEREFORE, do not ignore bond issues, council and mayoral elections, county positions, state office holders’ elections and only vote on presidential ballots. ALL VOTES MATTER!
Want to know more? Have a read:
From October, 2015, inGenere.it: “Intersectionality. Putting together
things that are often kept apart” by Jeff Hearn
http://www.ingenere.it/en/articles/intersectionality-putting-together-things-are-often-kept-apart
From February, 2015, NPR: “Study: Black Girls Are Being Pushed Out of School” by Karen Grigsby Bates
http://www.npr.org/sections/codeswitch/2015/02/13/384005652/study-black-girls-are-being-pushed-out-of-school
From February, 2015, the the Frisky: “18 Things White America Needs To Reconcile To Truly Become Colorblind” by Tiffanie Drayton
http://www.thefrisky.com/2015-02-26/18-things-white-america-needs-to-reconcile-to-truly-become-colorblind/
If you appreciated this series, please reblog/share it, comment, ask to be a guest blogger and contribute your own point of view or write on a related topic: http://www.sallyember.com
This third post was on advocacy and intersectionality (published on February 23, 2016, http://wp.me/p2bP0n-1C2).
The second was on food for indigent people in Missouri (published February 16, 2016, http://wp.me/p2bP0n-1BL).
The first one was on health care (published February 9, 2016, http://wp.me/p2bP0n-1By).

































You must be logged in to post a comment.