My Notes, Thoughts, Resources and Recommendations
for “Trauma-Informed” Education/Care
and ACEs (Adverse Childhood Experiences)
For those of us old enough to remember or who have studied sociology, psychology and/or education prior to 2000, there were precursors to this research: Risk Factors, which ACEs are a subset of, as well as Protective Factors and Resilience. For more about this important research, go here or https://youth.gov/youth-topics/youth-mental-health/risk-and-protective-factors-youth:
Relevant to ACEs are the Common Risk Factors for Childhood and Adolescent Problems, by Level of Influence

image from Devereux Center for Resilient Children
- Environmental Risk Factors Factors
—Laws and norms favorable to antisocial behavior
—Poverty and economic deprivation
—Low economic opportunity
—Neighborhood disorganization
—Low neighborhood attachment - Interpersonal and Social Risk Factors Factors
—Family communication and conflict
—Poor parent–child bonding
—Poor family management practices
—Family alcohol and drug use
—School failure
—Low commitment to school
—Rejection by conforming peer groups
—Association with antisocial peers - Individual Risk Factors Factors
—Family history of alcoholism
—Sensation-seeking orientation
—Poor impulse control
—Attention deficits
—Hyperactivity - Adapted from Fraser et al., 2004; Jenson & Howard, 1999; and Hawkins et al., 1998
from https://us.corwin.com/sites/default/files/upm-binaries/5975_Chapter_1_Jenson_Fraser__I_Proof.pdfSome heart-wrenching causation connections between childhood stress and adult medical problems have already been made:
—“…[M]ost adult women with fibromyalgia [emphasis mine]… have had stressful childhoods as reported by the journal, Stress and Health in 2009….The early chronic experience of stress appears to exert a much larger influence in contributing to the pain of fibromyalgia than any current stressful life event, as a 2006 study reported in the journal, Psychoneuroendocrinolgy. from http://medicalhealthnews.info/fibromyalgia-linked-childhood-stress-unprocessed-negative-emotions-2/The relationships between childhood experiences (“nurture”) and adult health have long been the subject of research. One precursor to ACEs research, for almost thirty years, the information derived from the biannual Youth Risk Behavior Survey (YRBSS) has been instrumental in determining what communities’ needs were, what prevention areas to focus upon, and how prevalent certain risky behaviors were over time because the USA government, in conjunction with state and municipal authories and school systems, began administering the YRBSS in 1990 and continues to this day, in odd years. Much of the data from the YRBSS overlaps with data needed and gathered about ACEs. See below.
The YRBSS (https://www.cdc.gov/healthyyouth/data/yrbs/overview.htm) was developed in 1990 to monitor priority health risk behaviors that contribute markedly to the leading causes of death, disability, and social problems among youth and adults in the United States. These behaviors, often established during childhood and early adolescence, include
- Behaviors that contribute to unintentional injuries and violence.
- Sexual behaviors related to unintended pregnancy and sexually transmitted infections, including HIV infection.
- Alcohol and other drug use.
- Tobacco use.
- Unhealthy dietary behaviors.
- Inadequate physical activity.
In addition, the YRBSS monitors the prevalence of obesity and asthma and other priority health-related behaviors plus sexual identity and sex of sexual contacts.
From 1991 through 2015, the YRBSS has collected data from more than 3.8 million high school students in more than 1,700 separate surveys.
ACEs research and subsequent work are building on all of these studies their data to help us advance in our understands, prevention, intervention and mitigation of trauma. The ACEs researchers began with this survey and its 10 categories (see below).
The 10 ACEs (Adverse Childhood Experiences) are, in summary form:

image from https://cdv.org/what-is-cdv/adverse-childhood-experiences/If you want to have each category be more fully defined (and some of them do include aspects you might not usually consider, so I recommend reviewing these if you haven’t, yet), go here, where you can actually “fill out” the survey at the same time:
https://www.ncjfcj.org/sites/default/files/Finding%20Your%20ACE%20Score.pdfHowever, if you find all this obvious, so is your score: you get one point for each of the ACEs that occurred in your childhood (before age 18 years old). The total of these = your ACEs score.
This ACEs number is important for examining the likelihood (statiscally speaking) of your having adverse consequences later in life (see below). The stats have three sections:
—> 0, 1 or 2 ACEs
—> 3 – 7 ACEs
—> more than 7 ACEsThe statistics tended to group in these ways in recognition of what types and how many negative consequences were most likely to occur for those with those ACEs numbers. Below is a description of the original study.
The Adverse Childhood Experiences (ACEs) Original Research:
“From 1995 to 1997, Kaiser Permanente’s Health Appraisal Clinic, in collaboration with Centers for Disease Control and Prevention, implemented one of the largest studies ever conducted on the origins of risk factors that have negative health and social consequences and the cumulative incidence and influence of psychological and physical abuse including: neglect, sexual abuse, witnessing violence, exposure to substance abuse, mental illness, suicidal behavior, and imprisonment of a family member (independent variables) on dependent variables that were measures of both mental health (depression, suicidality) and physical health (heart disease, cancer, chronic lung disease, skeletal fractures, liver disease, obesity) and health-related behaviors (alcoholism, drug abuse, smoking, high numbers of sexual partners) and poor self-rated health (Felitti et al. 1998).
“The ACE questionnaire was constructed using selected questions from published surveys (American Journal of Preventive Medicine, 2017). Prior to the survey there had been little study of the relationship between early childhood adverse experiences and adult medical problems and behaviors (Felitti et al. 1998).
“The ACE survey data was collected by mail from two waves of a sample of 17,000 adult members of Kaiser’s Health Maintenance Organization in San Diego, California between 1995 and 1997. The sample size itself was impressive. The release of the study findings was shocking to many when they showed the extent to which adverse childhood events negatively shaped future social and physical health outcomes, including life expectancy.
“Perhaps less surprising, the findings showed that the more negative events a child experienced the higher the likelihood s/he had as an adult of suffering an array of health and behavior problems including alcoholism, chronic pulmonary disease, depression, illicit drug use, liver disease, adolescent pregnancy and many more (Centers for Disease Control and Prevention 2014a, b). Further, adults with the highest level of ACEs had a life expectancy 20 years less than those without high levels of ACEs. The study sample did not consist primarily of low-income minority adults, a demographic often found to be “at risk.” It was mainly comprised of white, middle and upper income employed people; people who might be expected to have had more stable childhood environments because of parents’ employment and income.
“The original ACE study has generated more than 70 scientific articles, scores of conference presentations, and has shaped the design of research and as well as social programs. It is beyond the scope of this article to present a comprehensive review of the studies of the ACE survey, but ACEs Too High (2017) provides a list of ACE studies by year.
“Studies using the ACE questionnaire have expanded beyond Kaiser’s sample of white, HMO patients to include, for example, special populations such as children of alcoholics (Dube et al. 2001), and children with an incarcerated parent (Geller et al. 2009) and have found higher prevalences of ACEs than in the original Kaiser sample.
“ACE Studies of justice-involved populations (Baglivio et al. 2014; Messina and Grella 2006; Miller and Najavits 2012; Reavis et al. 2013) including juvenile justice-involved youth (Dierkhising et al. 2013) are raising awareness of the association of early childhood trauma and offender behaviors and needs, as are studies of justice-involved samples that include a focus on childhood trauma without using the ACE questionnaire (Wolff and Shi 2012). The studies consistently find elevated rates of childhood trauma in incarcerated populations and offender groups. For example, the Reavis et al. study (2013) of incarcerated males found ACE scores above 4 to be four times higher than in a normative male population.
“By bringing attention to the powerful impact that negative childhood experiences have on future health and functioning, the ACE study demonstrates the importance of gathering information early in the lives of children and their families and designing early intervention programs that target violence and neglect. It also points to the importance of collecting trauma histories from clients and highlights the essential role of prevention in program design. A particularly important contribution the Ace survey has made to offender and incarcerated groups is to emphasize the importance of trauma-targeted interventions in jails and prisons as well as in diversion programs.”
FMI: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5409906/
More about How ACEs Operate in Our Lives
This is a depiction of ACEs and their impacts in the form of a “pyramid of bad consequences”: if 3 or more ACEs form our lives’ “foundation,” we are much more likely to have a lot of other problems, including physical and mental health issues, suicidal ideation, criminal tendencies to the point of incarceration, and possible early death in our futures.
Even having 1 or 2 ACEs can wreck a person’s life and/or health if enough mitigating factors aren’t present, especially when the adverse experience was
—horrific,
—happened at a formative time, and/or
—was prolonged/repeated.
image from https://www.communitycommons.org/2014/08/aces-adverse-childhood-experiences/This excellent 2014 TEDMED talk on ACEs from a health care perspective
is on video, with presenter, Dr. Nadine Burke Harris, MDBurke offers the best summary of the study, its origins and findings, and their immediate and long-term applications for health care and other professionals as well as anyone affected by multiple ACEs.
“Childhood trauma isn’t something you just get over as you grow up. Pediatrician Nadine Burke Harris explains that the repeated stress of abuse, neglect and parents struggling with mental health or substance abuse issues has real, tangible effects on the development of the brain.
“This unfolds across a lifetime, to the point where those who’ve experienced high levels of trauma are at triple the risk for heart disease and lung cancer. An impassioned plea for pediatric medicine to confront the prevention and treatment of trauma, head-on.”
Worth your time to watch: https://www.ted.com/talks/nadine_burke_harris_how_childhood_trauma_affects_health_across_a_lifetime
ACEs High Scores Linked
to Adult Emotional and Physical Health ProblemsThere is a cycle regarding ACEs that usually occurs. Learning about how this cycle works is first. Then, figuring out how to intervene, interrupt and contravene the impacts can occur next.

image from https://dribbble.com/shots/2214296-Adverse-Childhood-Experiences-infographicKnow that Adverse Childhood Experiences (ACEs) are common
In case you were wondering about the prevalence of ACEs, here are some recent statistics from a small but supposedly representative sample and their source.
Of the 17,337 individuals surveyed, here is the prevalence of each possible adverse experience, from most to least, represented as a percentage:
—Physical abuse towards the child – 28.3%
—Substance abuse in the household – 26.9%
—Parental separation/divorce – 23.3%
—Sexual abuse toward the child – 20.7%
—Mental Illness in the household – 19.4%
—Emotional neglect towards the child – 14.8%
—Domestic violence in the household – 12.7%
—Emotional abuse towards the child – 10.6%
—Physical neglect towards the child – 9.9%
—Imprisoned household member – 4.7%ACEs are linked with a greater risk
of many problems in later lifeThese include:
- Alcohol abuse and dependence
- Early smoking initiation and current smoking status
- Illicit drug use
- IV drug abuse
- Obesity
- Suicide attempts
- Depression
- Anxiety
- Hyperactivity
- Sleep Disturbances
- Hallucinations
- Eating disorders
- Suicide attempts
- Post-traumatic stress disorder
- Conduct disorder
- Teen or unintended pregnancies
- Intimate partner violence
- Improper brain development
- Impaired learning ability and general cognitive difficulties
- Attention and memory difficulties
- Visual and/or motor impairment
- Lower language development
- Impaired social and emotional skills
- Poorer quality of life
Nikki Gratix offers more links and stats about ACEs and long-term effects, with our first glimmers of hope (link is below the text, here):
“Another long-term study indicated that approximately 80% of young adults who had previously been abused qualified for at least one psychiatric diagnosis at the age of 21 (Silverman, Reinherz & Gianconia, 1996).“Neglected or abused children are also
—59% more likely to be arrested during their childhood,
—28% more likely to engage in criminal behaviour as adults, and
—30% more likely to engage in violent crime as an adult (Widom & Maxfield, 2001).“Abuse and neglect during childhood can also negatively impact the ability of individuals to effectively establish and maintain healthy romantic adult relationships (Colman & Widom, 2004). As relationship warmth and social connection are key protective factors for long-term health and happiness, many of these greater risks could at least be partially explained by the greater risk of interpersonal conflict, disconnection and isolation.
“Individuals who have had negative experiences during their childhood can still grow and flourish as adults, and can also be more resilient as a result of learning how to overcome significant challenges when they are younger.
This diagram, below, depicts the Risk Factors, Protective Factors and Resilience interactive model clearly:

image from https://www.slideshare.net/PreventionWorks/bc-pc-december-13-2012, The InterdisciplinaryScience of Prevention Bernalillo County DWI Program Planning Council Meeting December 13, 2012 Frank G. Magourilos, MPS, CPS, ICPS Prevention Works“A major longitudinal study even found that what goes right during childhood is often more important than what goes wrong [emphasis mine], and having even one safe, stable and nurturing figure in a child’s life can reduce the later risk of psychological and physical health problems [emphasis mine] (Vaillant, 2015).
“Creating safe, stable and nurturing environments (SSNREs) is the key to having a positive impact on reducing ACEs going forward.”
LINK to the above: https://www.nikigratrix.com/silent-aces-epidemic-attachment-developmental-trauma/
FMI: “Steps to Create Safe, Stable, Nurturing Relationships and Environments,” 2014, https://www.cdc.gov/violenceprevention/pdf/essentials_for_childhood_framework.pdf
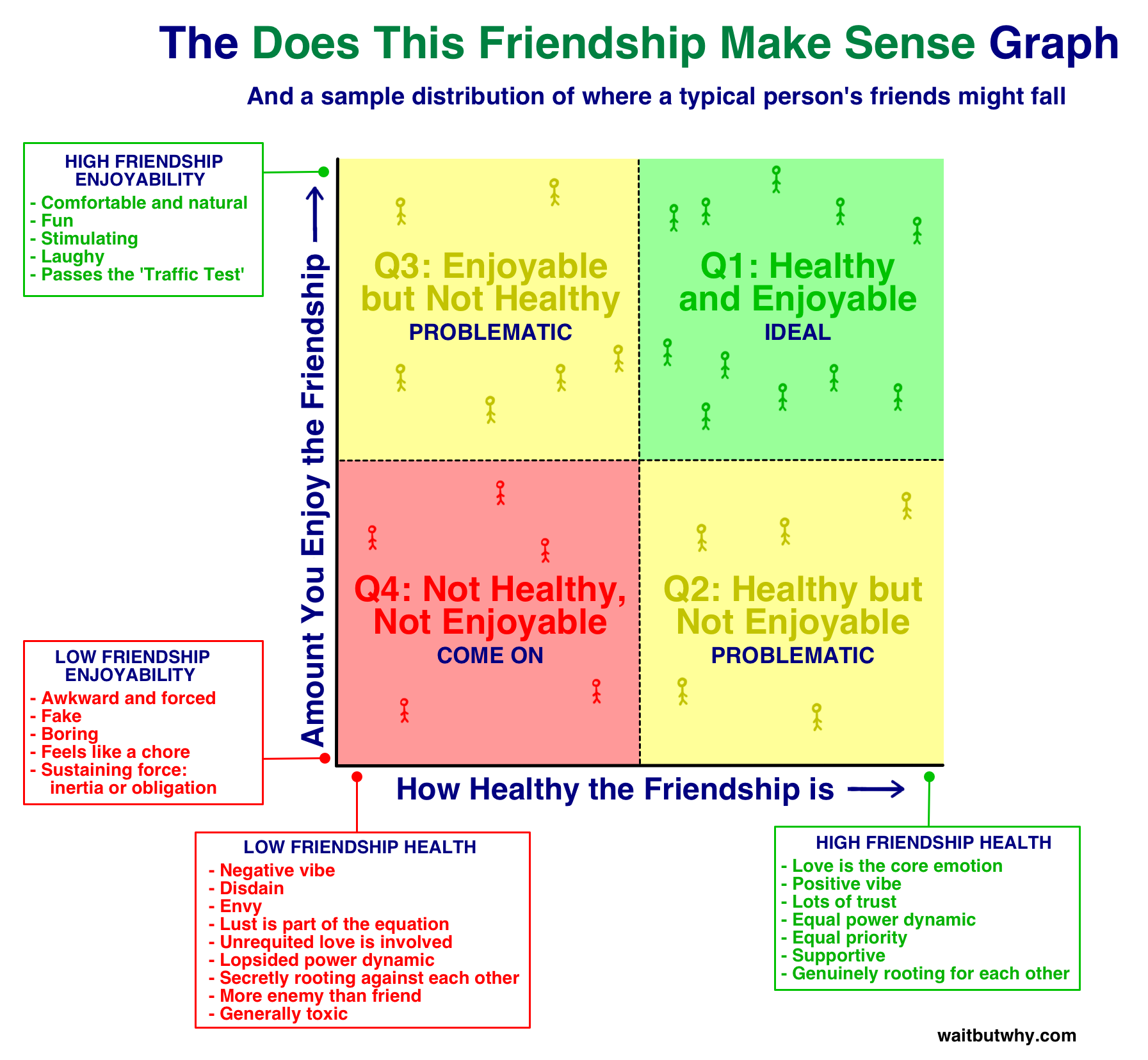
4 Quadrants/Types of Attachment:
I found this set of connections (below) to be a very helpful rubric for understanding the ways trauma impacts our ability to choose appropriate partners/friends, even colleagues and form positive relationships when we suffer from many ACEs because it brings in the main principles of John Bowlby‘s attachment theory quite intelligently.
- secure = consistent, responsive early care
= low anxiety, low avoidance
= positive views of self and others; comfortable relying on others, easily comforted - preoccupied = inconsistent early care
= high anxiety, low avoidance
negative view of selves but positive views of others; emotionally dependent, negative affects, hyper vigilance, low self-esteem - dismissive = early unresponsive care
= low anxiety, high avoidance
positive view of selves (see selves as resilient and not needing others), but negative views of others; uncomfortable with closeness, denial of attachment needs, avoidance of closeness, intimacy, dependency or close relationships; high self-reliance and independence - fearful = frequent rejection/abandonment by early caregivers
= high anxiety, high avoidance
seek social contact but inhibited by fear of rejection; approach/avoidance behavior in relationships; high negative affects and poor self-esteem
INTERVENTIONS & SOLUTIONS:
Trauma-Informed Care vs. Ordinary CareAs mentioned previously in this post, Protective Factors contribute to Resilience, and both are great predictors of how well a child or adult will do when affected by ACEs (or any other Risk Factors). The basic formula is that when any of the Risk Factors is present (and the higher the number, the worse the situation is for that person), increasing the number and types of Protective Factors for that person is very likely to increase their Resilience, which, in turn, decreases the likelihood that the person will succumb to peer pressure or inner motivation to engage in risky behaviors or fall victim to other risks and those consequences.
Similarly to Risk Factors (see above), researchers have divided Protective Factors into three categories: Individual, Family and Community
Researchers are also discovering that these same Protective Factors, particularly those that arise from within the Community and Individual (since Family is presumed to be the source/cause of the ACEs) can increase that person’s tendency toward Resilience, which then can mitigate the effects of ACEs as well.
Individual Protective Factors include:
—Positive physical development
—Academic achievement/intellectual development
—High self-esteem
—Emotional self-regulation
—Good coping skills and problem-solving skills
—Engagement and connections in two or more of the following contexts: school, with peers, in athletics, employment, religion, cultureFamily Protective Factors include:
—Family provides structure, limits, rules, monitoring, and predictability
—Supportive relationships with family members
—Clear expectations for behavior and valuesCommunity (School, Neighborhood, and Community) Protective Factors include:
—Presence of mentors and support for development of skills and interests
—Opportunities for engagement within school and community
—Positive norms
—Clear expectations for behavior
—Physical and psychological safety
from: https://youth.gov/youth-topics/youth-mental-health/risk-and-protective-factors-youthSome researchers have further divided these Factors into three age groupings: Early Childhood (ages newborn – 5 or 6 [school-age]), Childhood (ages 5 or 6 – 11 or 12 [ending before middle school or junior high school age]), and Adolescence (middle/junior high school and high school ages, 11 or 12 – 18). This classification is used to study each sector and period of a youth’s life more closely.

image from http://buncombeaces.org/“Once you know your ACEs score and its impact, there are personal strategies and community resources that exist to help you. Asking for help, developing trusting relationships, forming a positive attitude, and paying attention to your instincts and feelings are ways to improve your life. These can assist in breaking the cycle of ACEs in your family.
“Reaching out to a trusted member of your community such as a doctor, a counselor, a teacher, or a church or spiritual leader is another way to get help [emphsis mine]….Using these suggestions, both early in a child’s life and as an adult, can lessen the impact of ACEs on you and your family.”
10 Key Components of Trauma-Informed Care:

image from https://www.chcs.org/resource/10-key-ingredients-trauma-informed-care/“Trauma-Informed” (for educational settings, care, caregivers, institutions, youth programs, prisons, juvenile detention centers, court and police officers, etc.) is the newest way to describe what we MUST create and strengthen given our understanding of ACEs and the impacts of trauma throughout one’s lifetime. When society has better methods for prevention, we hope this won’t be as necessary. Until then, we are in dire need of more training, better programs, and more awareness.
https://www.rchc.net/wp-content/uploads/2017/08/Trauma-Informed-Care-slides.pdfResearch confirms that a person’s ability to Cope with trauma (and the neurodevelopmental effects) is rooted in the presence or absence of these circumstances and factors:
– Frequency – Single vs. repeated trauma (obviously, even one trauma is terrible, but more often is worse)
– Age when trauma occurred or began (the younger a person is, the worse off the person is likely to be)
– Agent – natural vs. human (weather disasters, earthquakes and fires are horribly traumatic, but war, interpersonal and domestic violence (being the victim OR the witness), and other human-inflicted harm are WORSE than “natural” causes of trauma when it comes to effects on the victims)
– Nature of the trauma – accidental vs. purposeful (particularly when the perpetrator was supposed to have been trustworthy and purported to “love” the victim, intentional harm is the worst type of trauma for a child)
– Environmental supports – Innate Resilience (there is some evidence in the fairly new field of epigenetics that some of us are “naturally” more resilient, particularly when it comes to resisting or lessening the effects of ACEs in the forms of bad health/diseases. Let’s find out WHY!)A lot of research on what contributes to resilience is happening NOW and recently.
From 2017, we can read: “Epigenetic Embedding of Early Adversity and Developmental Risk,” from Marla B. Sokolowski, PhD, F.R.S.C., W. Thomas Boyce, MD, Co-Directors of the Child and Brain Development Program, Canadian Institute for Advanced Research (CIFAR), Canada, who discovered: “[T]he embedding of adversity-related epigenetic marks is associated with increased susceptibility to compromised development and mental health….
“[A]dverse conditions in early childhood affect the number and placement of epigenetic marks on the DNA sequence. The developmental and health effects of early exposures to adversity and stress are socioeconomically partitioned, with children from the lower ranks of social class sustaining greater and more severe threats to normative development. Epigenetic processes that affect gene expression almost certainly have an impact on adversity-related, maladaptive outcomes….
“Adverse early childhood experiences can leave lasting marks on genes that are involved with stress responses, immunity and mental health, underscoring the importance of creating an optimal early childhood environment for each and every child.”
Other researchers created two categories of children to show the differences in fragility, “‘orchid children’…are more sensitive to both negative and positive environmental factors than their more resilient counterparts, called ‘dandelion children,'” which the above researchers utilized in their studies.
http://www.child-encyclopedia.com/epigenetics/according-experts/epigenetic-embedding-early-adversity-and-developmental-riskA great podcast/radio show, On Being, with host, Krista Tippett, provides many informative, entertaining and important audio experiences. This one is very relevant, here: RACHEL YEHUDA talks about “How Trauma and Resilience Cross Generations.”
“The new field of epigenetics sees that genes can be turned on and off and expressed differently through changes in environment and behavior. Rachel Yehuda is a pioneer in understanding how the effects of stress and trauma can transmit biologically, beyond cataclysmic events, to the next generation. She has studied the children of Holocaust survivors and of pregnant women who survived the 9/11 attacks.
“But her science is a form of power for flourishing beyond the traumas large and small that mark each of our lives and those of our families and communities [emphasis mine].”
Read the transcript and/or listen to podcast: https://onbeing.org/programs/rachel-yehuda-how-trauma-and-resilience-cross-generations-nov2017/
If you have more time and prefer the video format, Bruce McEwen, Ph.D., talks about “The Resilient Brain: Epigenetics, Stress and the Lifecourse,” at Cornell University in 2017.
For science geeks, this study is awesome! “Epigenetic modulation of inflammation and synaptic plasticity promotes resilience against stress in mice”: https://www.nature.com/articles/s41467-017-02794-5
“Three key neuroscience concepts are recommended for inclusion in Trauma-Informed Care programs and practices in ways that can enrich program design and guide the development of practical, Resilience -oriented interventions that can be evaluated for outcomes.
“A Resilience -oriented approach to TIC is recommended that moves from trauma information to neuroscience-based action with practical skills to build greater capacity for self-regulation and self-care in both service providers and clients.”
Another source of info about ACEs comes from this report, below (audio-only, with some text), from my former home-town public radio station, KRCB, in the North Bay, San Francisco Bay Area, California:

image from http://radio.krcb.org/post/educating-fellows-counter-adverse-childhood-experiences#stream/0Individual Protective Factors and Professional Training and Environmental Factors that Assist with Coping with ACEs are:
—Social support
—Supervision and consultation
—Resolution of one’s personal issues
—Strong ethical principles of practice
—Knowledge of theory
—On-going training
—Emotional intelligence/regulation
—Awareness of the potential and impact of Violent Trauma (VT).Then, of course, we have Oprah weighing in (finally) a few weeks ago:
Oprah’s 60 Minutes segment on ACES, 3/11/18

image from https://www.chcs.org/project/advancing-trauma-informed-care/Oprah (and others) talk about how we need to shift our focus from “What is wrong with you?” to “What happened to you?” with all traumatized individuals.
https://www.cbsnews.com/news/oprah-winfrey-treating-childhood-trauma/This video also mentions two important area of research about the brain and mental health related to ACEs or positive experiences. Good to know, but I’m still wanting more about what HELPS post-ACEs. Here we go!
“Winfrey speaks to Dr. Bruce Perry, a psychiatristand neuroscientist who authorities have consulted on high-profile events, such as school shootings. She also visits two organizations that treat their clients with the so-called “trauma-informed care” approach shaped by Dr. Perry. Both the agencies, SaintA and the Nia Imani Family Center, are in Milwaukee, where Winfrey spent part of her youth and experienced her own instances of childhood trauma.”
So, we know that chaos, threats, inconsistency, uncertainty, neglect, violence each constitutes a kind of traumas for children, and experiencing even one of these increases vulnerability in later life to many types of issues (academic, physical and mental health, interpersonal difficulties, employment problems).
That is the reason we need to move from focusing on consequences to preventing/mitigating early traumas/wounds.
One main “movement” is to bring in more institutions that provide “trauma-informed care.” Installing these changes is the best way to transform education, social and human services programming and treatment.
ACEs and I
I have written about ACEs before, disclosing that I have a very high ACEs score (9.5 out of 10). By the statistics reported since the early 1990s (see below), I should be in prison, institutionalized, or already dead. But, I’m not. Why is that?
Again, we need to ask “what happened?” rather than “what’s wrong?” to/with a child. Then, we need to build on strengths rather than focus on deficiencies or problems.
Why do some of us not have PTSD after many ACEs? Our reactions seem to be proportional to the numbers and frequency of whatever positive, protective, nurturing relationships we have had in early life. I am an example of an unusual case. See below.
I decided to look more deeply into this topic: what fosters Resilience? How do children and youth with high trauma scores not be completely unhealthy or miserable as adults? My discoveries are in this post and will keep coming.
Please comment on my site, on this post, regardless of where you’re reading this. The post is available starting 4/11/18: http://www.sallyember.com/blog or https://wp.me/p2bP0n-27w
Other Resources
Alice Miller‘s work = relevant because her main recommendation and research evidence are in alignment with ACEs’ researchers and therapists: it only takes ONE significant adult in a traumatized child’s life to greatly mitigate and even ameliorate the effects and later consequences of the trauma. I can attest to that truth.

Drama of the Gifted Child by Alice MillerHere is a great post about this book and Miller‘s work: https://www.psychologytoday.com/us/blog/suffer-the-children/201206/the-drama-the-gifted-child
Some local/regional resources (near both USA coasts), and more on their site, from CHCS (Center for Healthcare Strategies):
Center for Youth Wellness, San Francisco, CA, will implement adverse childhood experiences (ACE) screening, care coordination, and data management strategies to further its integrated care approach for addressing the physical and behavioral health needs of families with ACE exposure.
Greater Newark Healthcare Coalition, Newark, NJ, will establish care coordination, trauma screening and treatment, professional development, and data integration practices.
Montefiore Medical Group, Bronx, NY, will train all staff within its 22-practice outpatient ambulatory care network in trauma-informed approaches to care using a multi-disciplinary train-the-trainer model including patient representatives.
San Francisco Department of Public Health, San Francisco, CA, will develop a leadership model, learning community, and collaborative work group that will infuse trauma-informed systems’ principles and practices into public health and other child-, youth-, and family-serving agencies.
Stephen and Sandra Sheller 11th Street Family Health Services, Philadelphia, PA, will train all staff to adopt a standard approach to collective mindfulness practice and use an integrated mind-body treatment model in working with patients who have experienced trauma.
Women’s HIV Program at the University of California, San Francisco, CA, will develop a formal service integration partnership with the Trauma Recovery Center at San Francisco General Hospital to address the effects of lifetime trauma on adults.




















You must be logged in to post a comment.